

1 Introduction
Although aging is a natural process, it can be accompanied by some deleterious effects on functional fitness, with a reduction in physical capacities such as muscle power and cardiorespiratory capacity (Picca et al., 2018; Fragala et al., 2019). Especially when associated with physical inactivity, aging is related to an increase in plasma concentration of pro-inflammatory cytokines, a condition known as inflammaging, which may be related to the emergence or maintenance of several chronic diseases (Aiello et al., 2019; Flynn et al., 2019).
Aerobic and strength training and their combination (i.e., concurrent or combined training) are non-pharmacological approaches that can attenuate the deleterious aging effects (Garatachea et al., 2015). Regular physical training promotes increases in muscle strength (Vlietstra et al., 2018), power (Straight et al., 2016), cardiorespiratory fitness (Hurst et al., 2019), and quality of life (Awick et al., 2017; Campbell et al., 2021). Additionally, it reduces pro-inflammatory cytokines plasma concentration (Sardeli et al., 2018).
Functional Training (FT) uses resistance training with other stimuli, such as dynamic balance, motor coordination, flexibility, muscle power, and cardiorespiratory conditioning to increase the individual’s ability to perform activities of daily living (ADLs) safely and efficiently (Da Silva-Grigoletto et al., 2020; La Scala Teixeira et al., 2017).
A FT program can be an excellent approach for all older population, however, in the present study we chose post-menopausal women for some important reasons. Among them, the greater female representation in the older population. In 2030 women will comprise approximately 2/3 of older adults (He et al., 2016). Also, Alexandre et al. (2012) pointed out that older women are more susceptible to a decline in functional fitness. Another important aspect is reducing circulating hormones after menopause, mainly estrogen. This reduction is related to increased circulation of pro-inflammatory cytokines, such as interleukin-1 (IL-1), interleukin-6 (IL-6), and tumor necrosis factor (TNF-α) (Pfeilschifter et al., 2002). Concomitantly, pro-inflammatory cytokines could be a worse effect compromising postmenopausal women’s health and quality of life (Pfeilschifter et al., 2002; Monteiro Santiago et al., 2022).
The ideal dose of FT for postmenopausal women is not fully understood, as there are several variables to be considered for prescription, such as frequency, volume, and intensity. With reference to strength training dose, the current position of the National Strength and Conditioning Association (Fragala et al., 2019) recommends that older women perform between 1-3 sets per exercise and 1-2 multi-joint exercises for the main muscle groups. The intensity should range between 70%–85% of one maximum repetition (1RM). When maximum concentric speed is applied, the intensity should vary between 40%–60% of 1RM. A frequency of 2–3 times a week should be applied using a total of 8–10 multi-joint exercises per session, with the primary objective of stimulating the different components of physical fitness.
Based on the current guidelines, our research group showed increased functional fitness, from different strength parameters (i.e., isometric and dynamic strength) until functional tests similar to the ADLs (Aragão-Santos et al., 2019; Vasconcelos et al., 2020). Also, using FT, resistance training, and bodyweight training, we identified a reduction in pro-inflammatory cytokines (i.e., IL-6 and TNF-α) (Vasconcelos et al., 2020; Monteiro et al., 2022).
Despite the FT and other modalities’ benefits, there is no consensus about the optimal dose of exercise to promote the exercise’s benefits. With respect to resistance training volume, some studies pointed out the superior effects of multiple sets to increase muscle strength and improve body composition (Peterson et al., 2011; Borde et al., 2015). On the other hand, other studies have shown similar effects between single and multiple sets for this same outcome (Galvão and Taaffe, 2005; Radaelli et al., 2018; Cunha et al., 2020). To our best knowledge, no study has evaluated the effect of different FT volumes on functional fitness, muscle power and plasma cytokine concentrations in postmenopausal women.
Thus, we compared different FT volumes on postmenopausal women’s muscle power, functional fitness, and pro-inflammatory cytokines. Our initial hypothesis was that single-set (SSFT) and multiple-set (MSFT) protocols would induce similar effects on muscle power and functional fitness in the twelfth first weeks of training. After that, the MSFT would induce larger adaptations and reduces pro-inflammatory cytokines.
2 Materials and methods
2.1 Study design
A 26-week randomized controlled clinical trial was performed with 24 weeks of training (i.e., SSFT and MSFT) and 2 weeks for data collection of the dependent variables (i.e., functional fitness and blood samples) (Figure 1). This study followed the recommendations proposed by CONSORT (Schulz et al., 2010). Also, it was approved by the Research Ethics Committee (nº 2.947.316) and the Brazilian Registry of Clinical Trials (RBR-89KCHG).
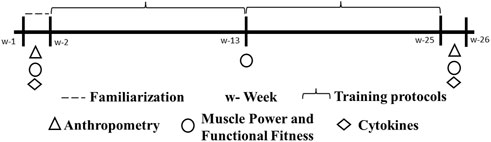
FIGURE 1. Experimental design.
2.2 Sample
The participants were recruited through leaflets, social media, and advertising. To be eligible to participate in the study, the participants should meet the following criteria: 60 years or older; do not practice any regular physical exercise in the 6 months before the beginning of the study; present a medical certificate indicating health requirements to perform physical activities. Also, the participants with the following conditions were excluded before the start of the training sessions: hypertension ≥ stage 2 (systolic ≥ 160 mmHg and diastolic ≥ 100 mmHg); cognitive impairment; musculoskeletal disorders that do not allow the practice of high-intensity exercises. All participants were informed about ethical standards, objectives, procedures, and risks related to the study and, after acceptance, signed the free and informed consent form.
Thus, 48 older women were randomly allocated to the Single-Set Functional Training (SSFT: n = 16), Multiple-Set Functional Training (MSFT: n = 16), and Control Group (CG: n = 16). The randomization was based on lower limb power values and the attribution of random numbers for each participant (Microsoft Office® 2016, Washington, United States). Thus, according to the random number, the participants were allocated to each group. A blinded independent researcher performed the allocation (Figure 2).
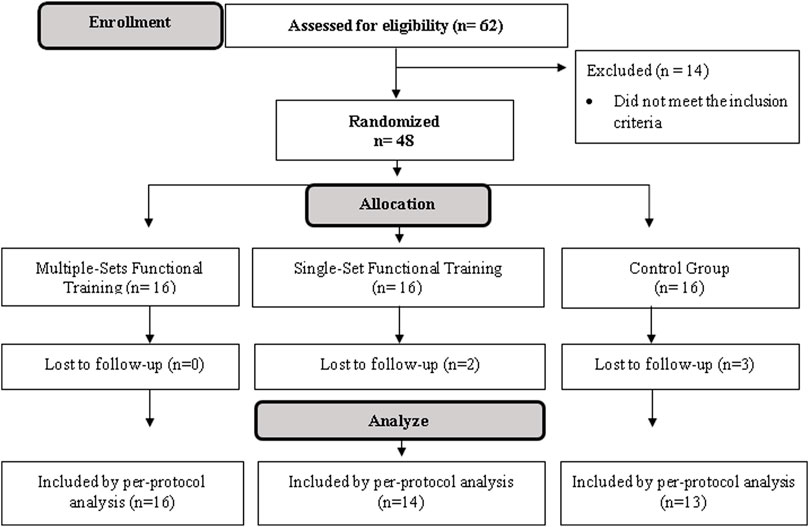
FIGURE 2. Flow diagram.
2.3 Exercise protocols
Following three familiarization training sessions, participants in the SSFT and MSFT groups underwent 72 training sessions conducted three times a week on non-consecutive days. The participants performed the exercises according to individual capacity. The effort was monitored and normalized during and after each workout defined by the OMNI-GSE scale (Da Silva-Grigoletto et al., 2013).
All participants performed specific exercises for their daily activities. Each session was divided into four parts: (1) mobility for the main joints (ankle, hip, and glenohumeral) and general warm-up exercises, including ten repetitions of squats and jumps lasting 5 min for SSFT and 10 min for MSFT; (2) intermittent activities, organized in a circuit stimulating agility, coordination, and muscle power (exercises: going up and down a step, alternating waves (rope), skipping, medicine ball throwing, moving between cones and jumping jacks) (OMNI-GSE: 6-7) lasting 6 min for SSFT and 12 min for MSFT; (3) multi-joint exercises organized in a circuit stimulating strength for the lower and upper limbs and intense spine stabilization (exercises: kettlebell lifting, suspension band row, 40 cm sit-up and stand-up, bilateral farmer’s walk, elasticized rowing, front floor plank, and pelvic lift) (OMNI-GSE: 7-8) lasting 8 min for SSFT and 16 min for MSFT.
In parts 2 and 3, the participants performed the exercises at maximum concentric speed. In all sessions, experienced physical education professionals supervised the participants to ensure the proper technique and safety. After the eighteenth session, a training progression was applied, so the external load was incremented in some exercises. In the exercises performed with their body mass, the participants were instructed to change the execution of the movement to achieve the proposed volume (i.e., 8 to 12 repetitions in each exercise). The training density was 30 s of work per 30 s of transition/recovery between stations.
In the 4th part (intermittent exercises), the participants performed a walk at a maximum speed in a 15 m course. Specifically, participants were separated into rows facing each other, with a distance of 15 m between them. The volunteers walked at maximum speed for 15 m and rested while the other participants performed the exercise. The total volume was 8–12 sprints per subject. This part lasted 3 min for SSFT and 6 min for MSFT. After the eighteenth session, the participants ran at maximum speed instead of walking.
Participants in the control group (CG) performed two sets of 15 s of static stretching per exercise (Nelson et al., 2007) for some body regions, such as the neck, shoulders, chest, back, arms, wrists, hands, hips, glutes, anterior thighs, posterior thighs, calves, and feet. All the exercises were performed with a submaximal range of motion and without great physical effort. A frequency of 3 weekly sessions and an average duration of 45 min per session was applied.
The exercise program followed conceptual aspects suggested by Resende-Neto et al. (2016) that were recently tested in some randomized controlled clinical trials (Aragão-Santos et al., 2019; Resende-Neto et al., 2019a; Vasconcelos et al., 2020). In addition, we added detailed descriptions of the exercises and progressions as Supplementary Material S1.
The training load was calculated using the following equation: rate of perceived exertion (RPE) x session duration in minutes (Falk Neto et al., 2020). Specifically, since we used an acceptable range of RPE, we have each group’s training load for the lower and upper limits of the RPE accepted. The only variable that differed between groups was the number of sets (SSFT = 1 and MSFT = 2). The number of exercises (14), repetitions range (8–12), and intensity (6-7 OMINI-GSE scale) were the same for both groups (Table 1).
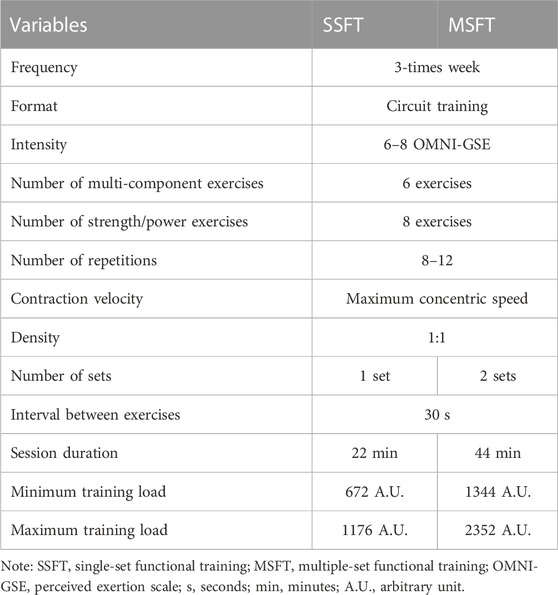
TABLE 1. Functional training variables.
2.4 Collection procedures
The functional fitness tests were applied before, after 12 weeks, and after 24 weeks of intervention. The tests were distributed over two consecutive days to minimize interference and with an interval of 2 days from the last training session after the 24 weeks of intervention. Besides the functional tests, before and post 24 weeks, blood samples were collected to measure cytokine plasma concentrations. Specifically, the blood samples were obtained at least 48 h before the first training session. After 24 weeks, the collection was made 1 week after the last training session to avoid bias in the basal cytokine levels. We emphasize that the evaluators were blind to the intervention performed by the participants.
2.4.1 Anthropometry
Body weight was assessed using a clinical scale (Filizola®, São Paulo, Brazil), with a maximum capacity of 150 kg. The height (cm) was measured with a stadiometer (Sanny, ES 2030, São Paulo, Brazil).
2.4.2 Muscle power
The muscle power was measured during the pushing and squatting actions performed in a Smith machine with three fixed external loads [Push (4, 8, and 12 kg) and Squat (10, 20, and 30 kg)]. The repetition velocity was measured using a linear encoder (speedometer) connected to the central unit of a data analysis program (Musclelab®, 3050e, Oslo, Norway), which made the conversion from velocity (meters per second) to muscle power (Watts). Initially, the participants warmed up by performing ten repetitions using just the barbel of the smith machine for the pushing action and with 5 kg beside the barbel for the squatting action at a moderate speed. After 3 min, they performed 3-5 repetitions at maximum concentric speed for each mentioned load. The repetition with the highest power produced was chosen as the final result (Lohne-Seiler et al., 2013). These measurements were used systematically in our research group’s studies and showed excellent reliability (Aragão-Santos et al., 2019; Vasconcelos et al., 2020).
2.4.3 Functional fitness tests
2.4.3.1 Putting on and taking off a T-shirt
The evaluator asked the participant to stand up with her arms extended at her sides with a large-sized T-shirt in her dominant hand. At the evaluator’s signal (“Go”), she put on the T-shirt entirely and immediately took it off, returning to the starting position (Vale et al., 2006). The participant performed two attempts with 1 min of rest between them, and the evaluator registered the shortest time for analysis. The participant was asked to perform the test again if she did not wear the T-shirt completely (Vale et al., 2006).
2.4.3.2 Gallon-jug shelf-transfer
This test aims to assess global functionality, emphasizing the upper limbs. The participant needed to move five-gallon jugs (3.9 kg each) from a lower (patella height) to an upper shelf (shoulder height) as quickly as possible. The participant was oriented to stand upright and stay laterally to a bookcase (2.13 m × 1.06 m with adjustable shelves). The evaluator showed how the test should be performed. Next, the participants were oriented to keep their back straight, always use the same hand to hold the gallon jugs, use the lower limbs to help with movement, and in case of discomfort or pain, stop the execution. One trial was made to correct possible mistakes. Two attempts were made to measure the execution time after the evaluator’s command (“prepare, now”) with 2 min of rest between them. We considered the shortest time for analysis and disqualified the attempt if the participant moved more than one gallon at a time or alternated hands to perform the movement (Signorile et al., 2007).
2.4.3.3 Standing up and walking around the house
This test assesses the individual’s agility and dynamic balance, using the functional movement of standing up from a sitting position and walking a certain distance with some changes of direction. Initially, a chair was centrally positioned between two cones at 4 m to the back and 3 m to the side of the chair, one cone positioned to the left and the other to the right. The participant started the test in a sitting position, with both feet off the ground, at the evaluator’s command (“Go!”) she needed to get up and walk to the cone on the right side, surround it, return along the same path, and sit down. Next, the participant needed to remove the feet from the ground, stand up, repeat the procedure for the left side, and finish seated with both feet off the ground. To complete one attempt, the participant should perform the abovementioned tasks twice (Dantas et al., 2014). The participant performed one familiarization and two attempts with 1 min of rest between them, and we recorded the shortest time for analysis (Dantas and Vale, 2004).
2.4.3.4 Five times sit-to-stand
In this test, we measured the participant’s ability to sit on and stand up from a chair as quickly as possible five times. This measure assesses functionality and is associated with the power of the lower limbs and the older person’s ability to react. During five consecutive movements, we instructed the volunteer to sit and stand up from a chair without using their arms. The test was timed from the evaluator’s command “go” until the individual sat down and stood up from the chair five times. Three to five hands-on trials were allowed to facilitate familiarity with the procedure. After this period, three attempts were performed, separated by 1 min each, with the shortest time recorded as the test value (Guralnik et al., 1994; Goldberg, 2012).
2.4.3.5 400-m walk
In this test, we instructed each participant to walk over 20 laps as fast as possible, without running, on a previously delimited 20-m course. The participant made only one attempt, and we recorded the execution time for further analysis (Vestergaard et al., 2009).
2.5 Cytokines assessment
Four milliliters of blood were collected by venipuncture to obtain at least 1.5 ml of serum. The blood was distributed into EDTA anticoagulant tubes, sodium citrate tubes, and serum separation accelerator tubes. Samples were centrifuged and frozen at −80°C until thawed for evaluation of immunological mediators. The cytokines serum concentrations were assessed by flow cytometry according to the manufacturer’s protocol to obtain measurements for interleukin (IL)-6, IL-10, and tumor necrosis factor (TNF)-α (Human TH1/TH2 CBA II Cytokine Kit, BD Biosciences®, San Diego, CA, United States). Briefly, lyophilized cytokine standards and serum samples were processed and analyzed using the BD FACS Calibur flow cytometer, FL4 channel. Three hundred events were acquired for each cytokine used. Data were analyzed using FCAP software, version 3.0 (BD Biosciences®, San Diego, CA, United States). Standard curves for each cytokine were generated using a classic mixture of mediators provided. The concentration in each serum sample was determined by interpolating the corresponding standard curve. The mean value obtained was considered whenever both kits evaluated a given cytokine. All calibration curves have a coefficient of linearity (R2) of 0.98 or greater (in many cases, 0.99). This coefficient ensured the test’s reliability. We found an intra-assay coefficient of variation of 26.2%.
2.6 Statistical analysis
We calculated the sample using the G*Power software (Erdfelder, Faul, and Buchner, 1996; Kiel, Germany—version 3.1.9.2) based on Aragão-Santos et al. (2019) results for the lower limb muscle power and cytokine values found by Tomeleri et al. (2018) and Vasconcelos et al. (2020). Specifically, we expected an average 10% increase in muscle power, a minimum 10% reduction in proinflammatory cytokines, used an α level of 0.05, and a power (1—β) of 0.80. Thus, we needed 36 volunteers (13 participants for each group) to attend the sample size estimation.
All data were analyzed using the Statistical Package for Social Sciences software (SPSS—version 22). We adopted a significance level of 5% (p ≤ 0.05) and expressed the results using means, standard deviation, and percentage of change. Homogeneity was tested using the Levene test. Normally distributed data were analyzed using repeated measures ANOVA (3×2) and Tukey’s multiple comparisons post-hoc test. Non-normally distributed data were analyzed using the Wilcoxon signed-rank test for within-group comparisons (pre vs. post) and the Kruskal-Wallis test for Between-groups (i.e., CG vs. SSFT vs. MSFT) comparisons. We used the delta for between-group comparisons (i.e., post-pre values per group). All tests were two-tailed, and we calculated the effect sizes (ES) according to the methodological procedures defined by Cohen (2009). The values were interpreted following: <0.19 insignificant; 0.20–0.49 small; 0.50–0.79 moderate; 0.80–1.29 large; >1.30 very large.
3 Results
There were no differences between groups at baseline for anthropometric and other characterization variables (Table 2).
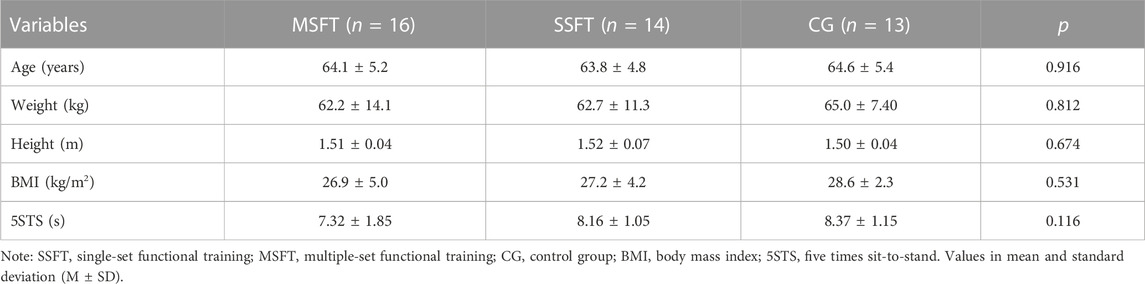
TABLE 2. Baseline characteristics of the participants.
The average participation rate was 85% (∼62 sessions) in MSFT and 95% (68 sessions) in SSFT.
Both groups increased upper limb power, but only the MSFT significantly improved (post-12 and post-24) compared to pre-intervention values in the bench press (4 kg). Respecting lower limb power, both MSFT and SSFT groups had significant improvement (post-12 and post-24) compared to pre-intervention for squat (10 kg). There were no significant differences between the groups (Table 3).
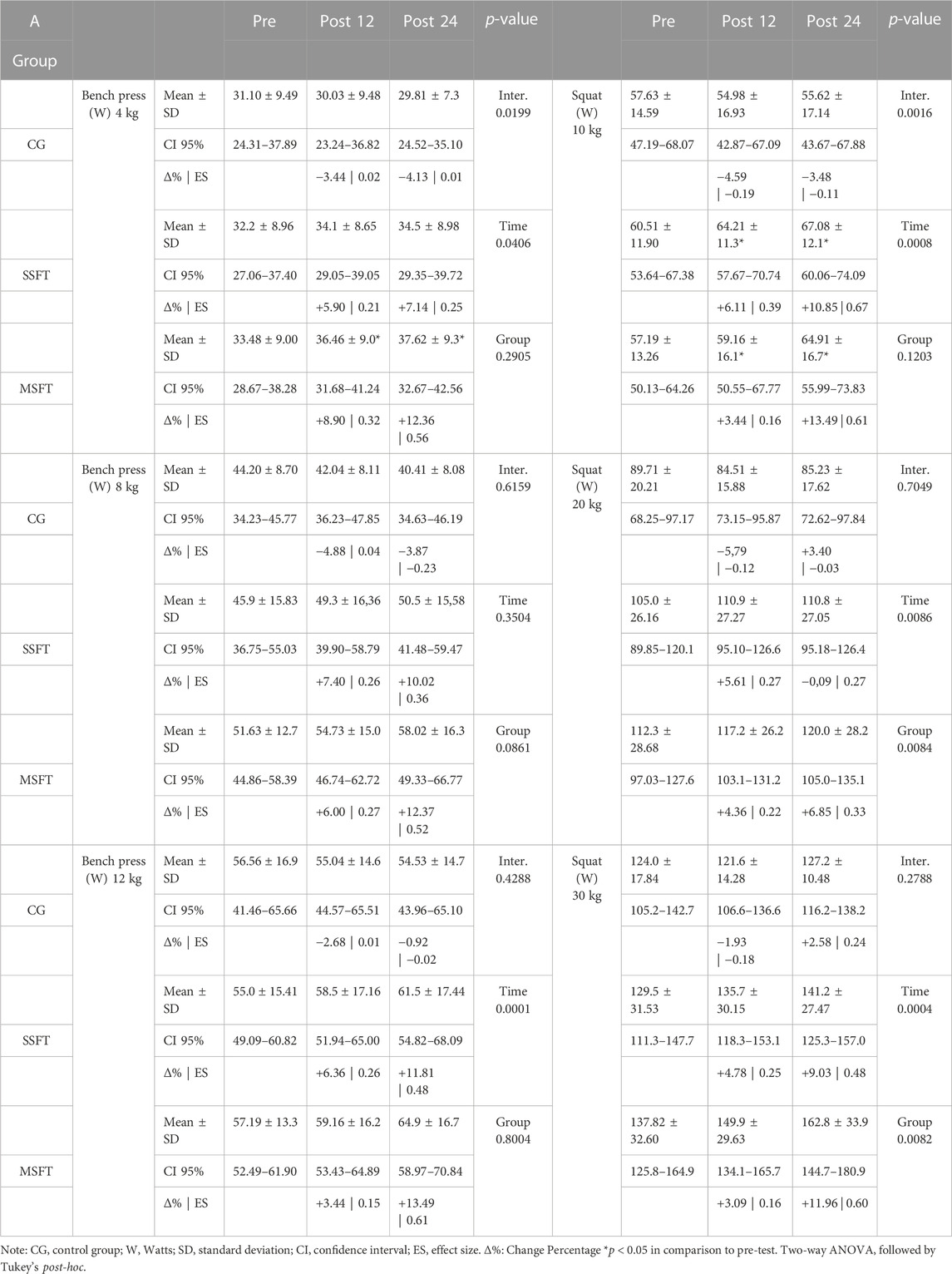
TABLE 3. Effect of Single-Set Functional Training (SSFT) and Multiple-Set Functional Training (MSFT) on upper and lower limb muscle power.
Between the MSFT and the SSFT, we detected a difference in the five times sit-to-stand test post 24 weeks of intervention for the MSFT compared to the SSFT (Figure 3D, p = 0.0117, ES: 0.29), however, training groups had no differences in the other functional tests. We identified only differences for time comparisons or compared to the CG. We did not find any effect in The Putting on and Taking off a T-Shirt test (Figure 3A).
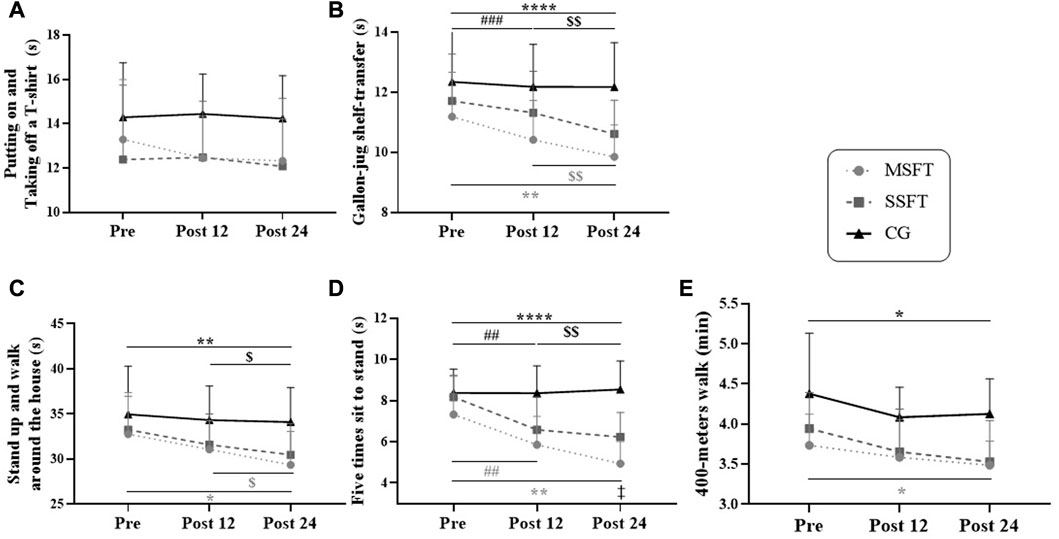
FIGURE 3. Values observed in functional fitness tests (A) putting on and taking off a T-shirt (B) gallon-jug shelf-transfer (C) standing up and walking around the house (D) five times sit-to-stand (E) 400-m walk) regarding the control group (CG, n = 13, black line with triangles), single-set functional training (SSFT, n = 14, grey dashed line with square), and multiple-set functional training (MSFT, n = 16, grey dotted line with circles) analyzed by repeated-measures ANOVA with two factors (time × group) and Tukey’s multiple comparisons. Note. Values expressed as mean and standard deviation; differences observed adopting p 0.05: *post24 vs. pre; $ post24 vs. post12; #post12 vs. pre; ‡ SSFT vs. MSFT. When p < 0.01: **; $$; ##. p< 0.001: ***; ###. p < 0.0001: ****.
We detected performance improvements in several functional tests in the MSFT group. Specifically, for the Gallon-jug shelf-transfer (Figure 3B), there was a time effect between pre vs. post-12, p = 0.0003, ES: 0.52; post-12 vs. post-24, p = 0.0089, ES: 0.43; pre vs. post-24, p < 0.0001, ES: 0.90. Also, we detect a time*group interaction effect with differences between MSFT post-12 vs. CG post-12, p = 0.0052, ES: 0.82; and MSFT post-24 vs. CG post-24, p = 0.0003, ES: 0.90). In the Standing up and walking around the house test (Figure 3C), we found a time effect for the MSFT between post-12 vs. post-24, p = 0.0113, ES: 0.53; pre vs. post-24, p < 0.0070, ES:0.73. Besides, we detected a time*group interaction effect between MSFT post24 vs. CG post24, p = 0.0149, ES: 0.81). For the test Five times sit-to-stand (Figure 3D), the MSFT had a time effect between pre vs. post-12, p = 0.0022, ES: 0.79; post-12 vs. post-24, p = 0.0031, ES: 0.65; pre vs. post-24, p < 0.0001, ES: 1.28. Also, we found a time*group interaction effect between MSFT post-12 vs. CG post-12, p = 0.0001, ES: 0.90; and MSFT post-24 vs. CGpost-24, p < 0.0001, ES: 0.98). Finally, for the 400-m walk test (Figure 3E), we noticed a time effect for the MSFT between pre vs. post24, p = 0.0188, ES: 0.64. Additionally, we detected a time*group interaction between MFST post-12 vs. CG post-12, p = 0.0176, ES: 0.78; and MFST post-24 vs. CG post-24, p = 0.0031, ES: 0.89).
In the SSFT group, we detected a time effect in Gallon-jug shelf-transfer (Figure 3B): post-12 vs. post-24, p = 0.0007, ES: 0.51; pre vs. post-24, p = 0.0022, ES: 0.70. Also, we found a time*group effect between SSFT post-24 vs. CG post-24, p = 0.0139, ES: 0.80. For the Standing up and walking around the house test we just detected a time effect (Figure 3C): post-12 vs. post-24, p = 0.0484, ES: 0.32; and pre vs. post-24, p = 0.0250, ES: 0.47). For the Five times sit-to-stand test, we detected a time and an interaction between time and group effects for the SSFT (Figure 3D): pre vs. post-12, p < 0.0001, ES: 1.51; pre vs. post-24, p < 0.0001, ES: 1.84; SSFT post-12 vs. CG post-12, p = 0.0111, ES: 0.80; and SSFT post-24 vs. CG post-24, p = 0.0003, ES: 0.89). Finally, we detected a time and interaction between time and group effects for SSFT in the 400-m walk test performances (Figure 3E): pre vs. post-24, p = 0.0326, ES: 0.91; and SSFT post-24 vs. CG post-24, p = 0.0158, ES: 0.80).
The p-values for two-way ANOVA of the functional tests were: Gallon-jug shelf-transfer (interaction: p = 0.0003, time: p < 0.0001, group: p = 0.0052); Standing up and walking around the house (interaction: p = 0.2178, time: p < 0.0001, group: p = 0.0667); Five times sit-to-stand (interaction: p < 0.0001, time: p < 0.0001, group: p < 0.0001); 400-m walk test (interaction: p = 0.6897, time: p = 0.0002, group: p = 0.0025), and Putting on and Taking off a T-Shirt (interaction: p = 0.4032, time: p = 0.2220, group: p = 0.0619).
We detected a time effect with a reduction in the MSFT for concentrations of TNF-α (p = 0.0002; ES: 0.70; Δ%: 66%) and IL-6 (p = 0.0026; ES: 0.51; Δ%: 45%). While the SSFT group only reduced concentrations of TNF-α (p = 0.0010; ES: 0.84; Δ%: 54%). We found no effect for IL-10 (MSFT, p = 0.8928, ES: 0.04, Δ%: 3.8%; SSFT, p = 0.3301; ES: 0.06, Δ%: 6.1%) (Figure 4).
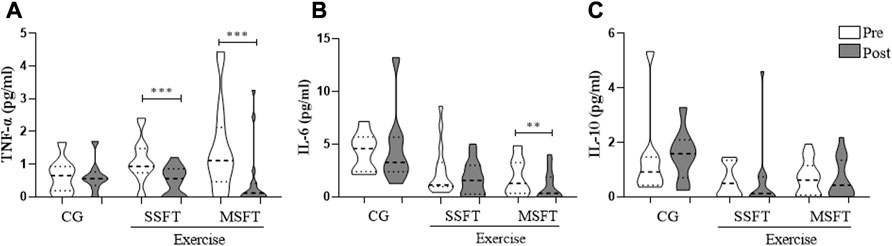
FIGURE 4. Plasma concentration of cytokines (A) TNF-α (B) IL-6 (C) IL-10 collected pre and post–24 weeks of Single–set functional training (SSFT), Multiple–set functional training (MSFT), or Control (CG). *p < 0.05 in comparison to the pre–test. Within–group comparisons (pre vs. post) based on Wilcoxon signed–rank test. Between–groups (i.e., CG, SSFT, and MSFT) comparisons based on the Kruskal–Wallis test. When p < 0.01: **; p value < 0.001: ***.
4 Discussion
The present study compared the effects of SSFT and MSFT on muscle power, functional fitness, and plasma cytokine concentrations in postmenopausal women over 24 weeks. The main finding was that both training groups produced a similar increase in muscle power and functional capacity after 12 weeks of intervention. Also, the MSFT promoted additional benefits after 24 weeks. These findings corroborated our initial hypothesis. Furthermore, it is the first study to assess different FT volumes’ effects on pro-inflammatory cytokines. Interestingly, our results demonstrated that SSFT and MSFT reduced TNF-α plasma concentration, and only the MSFT group decreased IL- 6.
Muscle power declines faster than maximal strength during aging, and this reduction contributes to lower functional fitness in older people (Byrne et al., 2016). In the present study, both intervention groups increased upper and lower limb muscle power. We only found a significant improvement in pushing (MSFT—bench press 4 kg) and squatting actions (MSFT and SSFT—squat 10 kg) at the lowest loads evaluated. One possible reason for this finding could be the functional training protocol, since part 2 (muscle power-oriented) was performed with smaller external loads or just the body mass. Additionally, the results produced by the MSFT could be derived from the higher volume applied to improve the upper limb power, since most of the training was focused on lower limb activities. SSFT and MSFT have common characteristics, such as multi-component work and maximum concentric speed, that may explain positive adaptations over time in lower limb muscle power (Ramírez-Campillo et al., 2014; Cadore and Izquierdo, 2018).
Our study is the first to compare the effects of different volumes of functional training on postmenopausal women. Our findings, however, corroborate other studies investigating different volumes’ effects using resistance training. Several articles indicated that both training protocols improved muscle function in postmenopausal and older women (Galvão and Taaffe, 2005; Abrahin et al., 2014) even though the larger volume group experienced greater improvements in specific functional tests.
We found no improvements in the upper limb’s functional fitness. One explanation could be related to the number of exercises focused on the upper limbs corresponding to 30% of the session. We designed the training protocol with a larger number of exercises for the lower limb because they are more affected by aging than the upper limbs (Larsson et al., 1979; Rikli and Jones, 2013). Thus, applying a greater volume of exercises for the upper limb could increase muscle strength and power. Additionally, according to Dantas et al. (2014) classification, our baseline values in the Putting on and Taking off a T-shirt test are classified as regular and good. Then, a greater stimulus should be applied to improve the performance in this test since our good initial participant’s level.
Although SSFT improved the Five times sit-to-stand test performance, the MSFT was superior, like previously published results (Ribeiro et al., 2015; Barbalho et al., 2017). The improvement in both groups could be attributed to the specificity of the squatting action and the higher number of lower limb exercises. Also, both groups performed the exercises at maximum concentric speed, stimulating muscle power (Byrne et al., 2016; Straight et al., 2016). Thus, likely the training stimuli increased the activation of type II muscle fibers, the excitability of alpha motor neurons in the spinal cord, and the recruitment and synchronization of motor units promoting more efficient adaptive responses in muscle power (Van Roie et al., 2020).
Both experimental groups significantly improved agility, coordination, dynamic balance, and global functionality, corroborating the current literature (Barbalho et al., 2017; Radaelli et al., 2018). The multi-component characteristic of our training protocol could explain the observed improvements in the functional fitness measures similar to daily activities (Resende-Neto et al., 2019b). In addition, regular exercise practice is associated with neural adaptations, such as increased motor unit recruitment, neural firing rate, and motor unit synchronization, promoting better performance the functional tests (Carroll et al., 2001; Kraemer and Ratamess, 2004; Lesinski et al., 2015; Schott et al., 2019; Wolf et al., 2020).
We found improvements for both training groups in aerobic endurance based on the 400-m walk test performance. The improvements were likely derived from the neuromuscular and metabolic training stimulus, such as the circuit-training session and the interval running in the last training part. Our findings corroborate Resende-Neto et al. (2016), which reported an 8% increase in the cardiorespiratory capacity of older women after a similar FT protocol.
Although physical exercise can reduce pro-inflammatory cytokines, there is no consensus about postmenopausal women (Macêdo Santiago et al., 2018; Sardeli et al., 2018; Flynn et al., 2019). For instance, Prestes et al. (2018) did not observe changes in circulating levels of IL-4 after 16 weeks of RT. IL-4 is an anti-inflammatory cytokine that plays an important role promoting muscle hypertrophy and antagonizes the activity of pro-inflammatory cytokines such as IL-6, TNF-α and IL-1β. Another study pointed out a reduction for C-reactive protein and TNF-α but not for IL-6 after 12 weeks of RT (Phillips et al., 2012). Similarly, Monteiro et al. (2022) found a reduction in TNF-α concentration induced by RT and bodyweight training after a 24-week intervention, with only the BWT decreasing IL-6.
Our findings corroborate Vasconcelos et al. (2020), that found an FT-induced reduction in TNF-α and IL-6 concentrations after 24 weeks of intervention. In the present trial, single-set training reduced TNF-α, a cytokine involved in the process of muscle breakdown and production of other cytokines, such as IL-6, that play a vital role in weakening muscle mass, strength, and power (Pfeilschifter et al., 2002; Vasconcelos et al., 2020).
It should be noted, however, that during and shortly after exercise, due to muscle contraction, IL-6 is produced and released by the muscle independently of TNF-α (Nieman et al., 1985; Forti et al., 2016). Acutely, increased IL-6 promotes higher hepatic glucose production during exercise, lipolytic action in skeletal muscle, regulation of insulin and glucose uptake by the muscle cell (Febbraio et al., 2004; Pedersen et al., 2007; Pedersen and Febbraio, 2012). Besides, IL-6 reduces low-grade chronic inflammation by stimulating inhibitory factors that limit the production of pro-inflammatory cytokines (e.g., IL-1 β and TNF-α) and stimulate the production of anti-inflammatory cytokines (e.g., IL-10) (Gleeson et al., 2011; Forti et al., 2016). Thus, muscle-derived IL-6 is associated with a lower risk of chronic diseases and premature deaths over time (Pedersen and Febbraio, 2012). Therefore, to avoid the possible acute effects of exercise on basal cytokines concentrations, we evaluated the cytokines only 1 week after the end of the exercise protocol.
In this study, only MSFT reduced IL-6. The greater training volume and, consequently, the higher muscle-derived IL-6 concentration during and after training could have generated an anti-inflammatory environment. The already mentioned muscle-derived IL-6 effects in response to exercise support this hypothesis. Also, a meta-analysis with older diabetic adults pointed out that longer programs or a higher number of sessions demonstrated larger IL-6 reductions (Hayashino et al., 2014). Another possible explanation for the IL-6 declines could be associated with body composition changes since muscle hypertrophy, or lower fat mass could favor the reduction of these pro-inflammatory markers (Sardeli et al., 2018). We did not evaluate these variables, which is a limitation of our study. We pointed out, however, reductions in pro-inflammatory cytokines, an important finding related to the quality of life and reduced morbidity (Flynn et al., 2019). Much like Vasconcelos et al. (2020), we found no modulation of this cytokine after a TF protocol. IL-10 modulation is a controversial result, with other studies also demonstrating no differences in concentration after training programs (Campo et al., 2015).
Our study provides an important practical application, since time constraints had been reported as one of the main barriers to exercise adherence (Schutzer, 2004; Aily et al., 2017). Besides, high-volume protocols were associated with higher abandonment rates (Hass et al., 2000). Thus, an effective time-efficient protocol using a single set approach could be an excellent strategy to promote benefits in the functional fitness of postmenopausal women. Furthermore, SSFT can be applied to community programs, as it allows more participants per hour of intervention.
5 Conclusion
SSFT and MSFT promote similar muscle power and functional fitness improvements over 24 weeks. Only MSFT reduces TNF-α and IL-6, while SSFT only decreases TNF-α levels. These findings can help professionals in choosing the training volume for postmenopausal women.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Research Ethics Committee (n°2.947.316) and by the Brazilian Registry of Clinical Trials (RBR-89KCHG). The patients/participants provided their written informed consent to participate in this study.
Author contributions
JR and AV: Conceptualization, formal analysis, methodology, data curation, writing. JA-S: Conceptualization, methodology, writing. AR-N: Data curation, investigation, supervision. MM: Formal analysis, visualization, investigation. AN: Formal analysis, visualization, investigation. AC: Formal analysis, visualization, investigation. CC: Formal analysis, visualization, investigation, methodology, supervision. TM: Formal analysis, visualization, investigation, methodology, supervision. MD-G: Investigation, Methodology, supervision, data curation. The authors declare that they contributed significantly to the experimental design, data analysis, and manuscript preparation.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
Acknowledgments
The authors thank the Functional Training Group (FTG by UFS) from the Department of Physical Education of the Federal University of Sergipe for technical and methodological support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2023.1054424/full#supplementary-material
References
Abrahin, O., Rodrigues, R. P., Nascimento, V. C., Da Silva-Grigoletto, M. E., Sousa, E. C., and Marçal, A. C. (2014). Single- and multiple-set resistance training improves skeletal and respiratory muscle strength in elderly women. Clin. Interventions Aging 9, 1775–1782. doi:10.2147/CIA.S68529
CrossRef Full Text | Google Scholar
Aiello, A., Farzaneh, F., Candore, G., Caruso, C., Davinelli, S., Gambino, C. M., et al. (2019). Immunosenescence and its hallmarks: How to oppose aging strategically? A review of potential options for therapeutic intervention. Front. Immunol. 10, 2247. doi:10.3389/fimmu.2019.02247
PubMed Abstract | CrossRef Full Text | Google Scholar
Aily, J. B., Carnaz, L., Farche, A. C. S., and Takahashi, A. C. de M. (2017). Perception of barriers to physical exercise in women population over 60. Mot. Rev. Educ. Física 23. doi:10.1590/s1980-6574201700020012
CrossRef Full Text | Google Scholar
Alexandre, T. da S., Corona, L. P., Nunes, D. P., Santos, J. L. F., Duarte, Y. A. de O., Lebrao, M. L., et al. (2012). Gender differences in incidence and determinants of disability in activities of daily living among elderly individuals: SABE study. J. Arch. Gerontol. Geriatr 55, 431–437. doi:10.1016/j.archger.2012.04.001
CrossRef Full Text | Google Scholar
Aragão-Santos, J. C., De Resende-Neto, A. G., Nogueira, A. C., Feitosa-Neta, M. de L., Brandão, L. H., Chaves, L. M., et al. (2019). The effects of functional and traditional strength training on different strength parameters of elderly women: A randomized and controlled trial. J. Sports Med. Phys. Fit. 59, 380–386. doi:10.23736/S0022-4707.18.08227-0
CrossRef Full Text | Google Scholar
Awick, E. A., Ehlers, D. K., Aguiñaga, S., Daugherty, A. M., Kramer, A. F., and McAuley, E. (2017). Effects of a randomized exercise trial on physical activity, psychological distress and quality of life in older adults. Gen. Hosp. Psychiatry 49, 44–50. doi:10.1016/j.genhosppsych.2017.06.005
PubMed Abstract | CrossRef Full Text | Google Scholar
Barbalho, M. de S. M., Gentil, P., Izquierdo, M., Fisher, J., Steele, J., and Raiol, R. de A. (2017). There are no no-responders to low or high resistance training volumes among older women. Exp. Gerontol. 99, 18–26. doi:10.1016/j.exger.2017.09.003
PubMed Abstract | CrossRef Full Text | Google Scholar
Borde, R., Hortobágyi, T., and Granacher, U. (2015). Dose–response relationships of resistance training in healthy old adults: A systematic review and meta-analysis. Sports Med. 45, 1693–1720. doi:10.1007/s40279-015-0385-9
PubMed Abstract | CrossRef Full Text | Google Scholar
Byrne, C., Faure, C., Keene, D. J., and Lamb, S. E. (2016). Ageing, muscle power and physical function: A systematic review and implications for pragmatic training interventions. Sports Med. 46, 1311–1332. doi:10.1007/s40279-016-0489-x
PubMed Abstract | CrossRef Full Text | Google Scholar
Cadore, E. L., and Izquierdo, M. (2018). Muscle power training: A hallmark for muscle function retaining in frail clinical setting. J. Am. Med. Dir. Assoc. 19, 190–192. doi:10.1016/j.jamda.2017.12.010
PubMed Abstract | CrossRef Full Text | Google Scholar
Campbell, E., Petermann-Rocha, F., Welsh, P., Celis-Morales, C., Pell, J. P., Ho, F. K., et al. (2021). The effect of exercise on quality of life and activities of daily life in frail older adults: A systematic review of randomised control trials. Exp. Gerontol. 147, 111287. doi:10.1016/j.exger.2021.111287
PubMed Abstract | CrossRef Full Text | Google Scholar
Campo, R. A., Light, K. C., O’Connor, K., Nakamura, Y., Lipschitz, D., LaStayo, P. C., et al. (2015). Blood pressure, salivary cortisol, and inflammatory cytokine outcomes in senior female cancer survivors enrolled in a tai chi chih randomized controlled trial. J. Cancer Surviv. 9, 115–125. doi:10.1007/s11764-014-0395-x
PubMed Abstract | CrossRef Full Text | Google Scholar
Carroll, T. J., Riek, S., and Carson, R. G. (2001). Neural adaptations to resistance training: Implications for movement control. Sports Med. 31, 829–840. doi:10.2165/00007256-200131120-00001
PubMed Abstract | CrossRef Full Text | Google Scholar
Cohen, J. (2009). Statistical power analysis for the behavioral sciences. New York, NY: Psychology Press.
Google Scholar
Cunha, P. M., Nunes, J. P., Tomeleri, C. M., Nascimento, M. A., Schoenfeld, B. J., Antunes, M., et al. (2020). Resistance training performed with single and multiple sets induces similar improvements in muscular strength, muscle mass, muscle quality, and IGF-1 in older women: A randomized controlled trial. J. Strength Cond. Res. 34, 1008–1016. doi:10.1519/JSC.0000000000002847
PubMed Abstract | CrossRef Full Text | Google Scholar
Da Silva-Grigoletto, M. E., Montaner, B. H. V., Heredia, J., Ordóñez, F. M., Brito, P., Vaamonde, D., et al. (2013). Validación de la escala de valoración subjetiva del esfuerzo OMNI-GSE para el control de la intensidad global en sesiones de objetivos múltiples en personas mayores. Kronos Rev. Univ. Act. Física El Deporte 12, 32–40.
Google Scholar
Da Silva-Grigoletto, M. E., Resende-Neto, A. G., and Teixeira, C. V. L. S. (2020). Treinamento funcional: uma atualização conceitual. Rev. Bras. Cineantropom. Desempenho Hum. 22, e70646. doi:10.1590/1980-0037.2020v22e72646
CrossRef Full Text | Google Scholar
Dantas, E. H., Figueira, H. A., Emygdio, R. F., and Vale, R. G. (2014). Functional autonomy GdlAm protocol classification pattern in elderly women. Indian J. Appl. Res. 4, 262–266. doi:10.15373/2249555x/july2014/159
CrossRef Full Text | Google Scholar
Dantas, E. H., and Vale, R. G. (2004). Protocolo GDLAM de avaliação da autonomia funcional. Fit. Perform. J. 3, 175–183. doi:10.3900/fpj.3.3.175.p
CrossRef Full Text | Google Scholar
Falk Neto, J. H., Tibana, R. A., de Sousa, N. M. F., Prestes, J., Voltarelli, F. A., and Kennedy, M. D. (2020). Session rating of perceived exertion is a superior method to monitor internal training loads of functional fitness training sessions performed at different intensities when compared to training impulse. Front. physiology 11, 919. doi:10.3389/fphys.2020.00919
CrossRef Full Text | Google Scholar
Febbraio, M. A., Hiscock, N., Sacchetti, M., Fischer, C. P., and Pedersen, B. K. (2004). Interleukin-6 is a novel factor mediating glucose homeostasis during skeletal muscle contraction. Diabetes 53, 1643–1648. doi:10.2337/diabetes.53.7.1643
PubMed Abstract | CrossRef Full Text | Google Scholar
Flynn, M. G., Markofski, M. M., and Carrillo, A. E. (2019). Elevated inflammatory status and increased risk of chronic disease in chronological aging: Inflamm-aging or inflamm-inactivity? Aging Dis. 10, 147–156. doi:10.14336/AD.2018.0326
PubMed Abstract | CrossRef Full Text | Google Scholar
Forti, L. N., Roie, E. V., Njemini, R., Coudyzer, W., Beyer, I., Delecluse, C., et al. (2016). Load-specific inflammation mediating effects of resistance training in older persons. JAMDA 17, 547–552. doi:10.1016/j.jamda.2016.02.010
PubMed Abstract | CrossRef Full Text | Google Scholar
Fragala, M. S., Cadore, E. L., Dorgo, S., Izquierdo, M., Kraemer, W. J., Peterson, M. D., et al. (2019). Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 33, 2019–2052. doi:10.1519/JSC.0000000000003230
PubMed Abstract | CrossRef Full Text | Google Scholar
Galvão, D. A., and Taaffe, D. R. (2005). Resistance exercise dosage in older adults: Single- versus multiset effects on physical performance and body composition. Am. Geriatrics Soc. 53, 2090–2097. doi:10.1111/j.1532-5415.2005.00494.x
CrossRef Full Text | Google Scholar
Garatachea, N., Pareja-Galeano, H., Sanchis-Gomar, F., Santos-Lozano, A., Fiuza-Luces, C., Morán, M., et al. (2015). Exercise attenuates the major hallmarks of aging. Rejuvenation Res. 18, 57–89. doi:10.1089/rej.2014.1623
PubMed Abstract | CrossRef Full Text | Google Scholar
GleesonBishop, M,N. C., Stensel, D. J., Lindley, M. R., Mastana, S. S., and Nimmo, M. A. (2011). The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 11, 607–615. doi:10.1038/nri3041
PubMed Abstract | CrossRef Full Text | Google Scholar
Goldberg, A. (2012). The five-times-sit-to-stand-test (FTSST), the short version of the activities-specific balance confidence (ABC) scale, and fear of falling predict step execution time (SET) in older adults. Archives Gerontology Geriatrics 54, 434–438. doi:10.1016/j.archger.2011.06.017
CrossRef Full Text | Google Scholar
Guralnik, J. M., Simonsick, E. M., Ferrucci, L., Glynn, R. J., Berkman, L. F., Blazer, D. G., et al. (1994). A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 49, M85–M94. doi:10.1093/geronj/49.2.m85
PubMed Abstract | CrossRef Full Text | Google Scholar
Hass, C. J., Garzarella, L., De Hoyos, D., and Pollock, M. L. (2000). Single versus multiple sets in long-term recreational weightlifters. Med. Sci. Sports Exerc. 235, 235–242. doi:10.1097/00005768-200001000-00035
PubMed Abstract | CrossRef Full Text | Google Scholar
Hayashino, Y., Jackson, J. L., Hirata, T., Fukumori, N., Nakamura, F., Fukuhara, S., et al. (2014). Effects of exercise on C-reactive protein, inflammatory cytokine and adipokine in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Metabolism 63, 431–440. doi:10.1016/j.metabol.2013.08.018
PubMed Abstract | CrossRef Full Text | Google Scholar
He, W., Goodkind, D., and Kowal, P. (2016). An Aging World: 2015. United States Census Bureau.
Hurst, C., Weston, K. L., McLaren, S. J., and Weston, M. (2019). The effects of same-session combined exercise training on cardiorespiratory and functional fitness in older adults: A systematic review and meta-analysis. Aging Clin. Exp. Res. 31, 1701–1717. doi:10.1007/s40520-019-01124-7
PubMed Abstract | CrossRef Full Text | Google Scholar
Kraemer, W. J., and Ratamess, N. A. (2004). Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 36, 674–688. doi:10.1249/01.MSS.0000121945.36635.61
PubMed Abstract | CrossRef Full Text | Google Scholar
La Scala Teixeira, C. V., Evangelista, A. L., Novaes, J. S., Da Silva Grigoletto, M. E., and Behm, D. G. (2017). You’re only as strong as your weakest link”: A current opinion about the concepts and characteristics of functional training. Front. Physiol. 8, 643. doi:10.3389/fphys.2017.00643
PubMed Abstract | CrossRef Full Text | Google Scholar
Larsson, L., Grimby, G., and Karlsson, J. (1979). Muscle strength and speed of movement in relation to age and muscle morphology. J. Appl. Physiol. 46, 451–456. doi:10.1152/jappl.1979.46.3.451
PubMed Abstract | CrossRef Full Text | Google Scholar
Lesinski, M., Hortobágyi, T., Muehlbauer, T., Gollhofer, A., and Granacher, U. (2015). Effects of balance training on balance performance in healthy older adults: A systematic review and meta-analysis. Sports Med. 45, 1721–1738. doi:10.1007/s40279-015-0375-y
PubMed Abstract | CrossRef Full Text | Google Scholar
Lohne-Seiler, H., Torstveit, M. K., and Anderssen, S. A. (2013). Traditional versus functional strength training: Effects on muscle strength and power in the elderly. J. Aging Phys. Act. 21, 51–70. doi:10.1123/japa.21.1.51
PubMed Abstract | CrossRef Full Text | Google Scholar
Macêdo Santiago, L. Â., Neto, L. G. L., Borges Pereira, G., Leite, R. D., Mostarda, C. T., de Oliveira Brito Monzani, J., et al. (2018). Effects of resistance training on immunoinflammatory response, TNF-alpha gene expression, and body composition in elderly women. J. Aging Res. 2018, 1467025–1467110. doi:10.1155/2018/1467025
PubMed Abstract | CrossRef Full Text | Google Scholar
Monteiro, M. R. P., Aragão-Santos, J. C., Vasconcelos, A. B. S., De Resende-Neto, A. G., Da Silva Chaves, L. M., Alan Pantoja Cardoso, A. P., et al. (2022). Bodyweight and combined training reduce chronic low-grade inflammation and improve functional fitness of postmenopausal women. Sports 10, 143. doi:10.3390/sports10100143
PubMed Abstract | CrossRef Full Text | Google Scholar
Nelson, A. G., Kokkonen, J., and Pinheiro, M. F. O. (2007). Anatomia do alongamento guia ilustrado para aumentar a flexibilidade e a força muscular. Barueri: Manole.
Google Scholar
Nieman, D. C., Henson, D. A., Smith, L. L., Utter, A. C., Vinci, D. M., Davis, J. M., et al. (1985). Cytokine changes after a Marathon race. J. Appl. Physiol. 91, 109–114. doi:10.1152/jappl.2001.91.1.109
CrossRef Full Text | Google Scholar
Pedersen, B. K., Akerström, T. C., Nielsen, A. R., and Fischer, C. P. (2007). Role of myokines in exercise and metabolism. J. Appl. Physiol. 103 (3), 1093–1098. doi:10.1152/japplphysiol.00080.2007
PubMed Abstract | CrossRef Full Text | Google Scholar
Peterson, M. D., Pistilli, E., Haff, G. G., Hoffman, E. P., and Gordon, P. M. (2011). Progression of volume load and muscular adaptation during resistance exercise. Eur. J. Appl. Physiol. 111, 1063–1071. doi:10.1007/s00421-010-1735-9
PubMed Abstract | CrossRef Full Text | Google Scholar
Pfeilschifter, J., Koditz, R., Pfohl, M., and Schatz, H. (2002). Changes in proinflammatory cytokine activity after menopause. Endocr. Rev. Feb 23 (1), 90–119. doi:10.1210/edrv.23.1.0456
CrossRef Full Text | Google Scholar
Phillips, M. D., Patrizi, R. M., Cheek, D. J., Wooten, J. S., Barbee, J. J., and Mitchell, J. B. (2012). Resistance training reduces subclinical inflammation in obese, postmenopausal women. Am. Coll. Sports Med. 44, 2099–2110. doi:10.1249/MSS.0b013e3182644984
CrossRef Full Text | Google Scholar
Picca, A., Calvani, R., Bossola, M., Allocca, E., Menghi, A., Pesce, V., et al. (2018). Update on mitochondria and muscle aging: All wrong roads lead to sarcopenia. Biol. Chem. 399 (5), 421–436. doi:10.1515/hsz-2017-0331
PubMed Abstract | CrossRef Full Text | Google Scholar
Prestes, J., Nascimento, D. C., Neto, I. V. S., Tibana, R. A., Shiguemoto, G. E., De Andrade Perez, S. E., et al. (2018). The effects of muscle strength responsiveness to periodized resistance training on resistin, leptin and cytokine in elderly post-menopausal women Running Head: Responsiveness and Periodization in Elderly. J. Strength Cond. Res. 32, 113–120. doi:10.1519/JSC.0000000000001718
PubMed Abstract | CrossRef Full Text | Google Scholar
Radaelli, R., Brusco, C. M., Lopez, P., Rech, A., Machado, C. L. F., Grazioli, R., et al. (2018). Higher muscle power training volume is not determinant for the magnitude of neuromuscular improvements in elderly women. Exp. Gerontol. 110, 15–22. doi:10.1016/j.exger.2018.04.015
PubMed Abstract | CrossRef Full Text | Google Scholar
Ramírez-Campillo, R., Castillo, A., de la Fuente, C. I., Campos-Jara, C., Andrade, D. C., Álvarez, C., et al. (2014). High-speed resistance training is more effective than low-speed resistance training to increase functional capacity and muscle performance in older women. Exp. Gerontol. 58, 51–57. doi:10.1016/j.exger.2014.07.001
PubMed Abstract | CrossRef Full Text | Google Scholar
Resende-Neto, A. G., do Nascimento, M. A., De Sá, C. A., Ribeiro, A. S., Desantana, J. M., and Da Silva-Grigoletto, M. E. (2019b). Comparison between functional and traditional training exercises on joint mobility, determinants of walking and muscle strength in older women. J. Sports Med. Phys. Fit. 59, 1659–1668. doi:10.23736/S0022-4707.19.09751-2
CrossRef Full Text | Google Scholar
Resende-Neto, A. G., Aragão-Santos, J. C., Oliveira-Andrade, B. C., Silva Vasconcelos, A. B., De Sá, C. A., Aidar, F. J., et al. (2019a). The efficacy of functional and traditional exercise on the body composition and determinants of physical fitness of older women: A randomized crossover trial. J. Aging Res. 2019, 5315376–5315379. doi:10.1155/2019/5315376
PubMed Abstract | CrossRef Full Text | Google Scholar
Resende-Neto, A. G. de, Feitosa Neta, M. de L., Santos, M. S., La Scala Teixeira, C. V., De Sá, C. A., and Da Silva-Grigoletto, M. E. (2016). Functional training versus traditional strength training: Effects on physical fitness indicators in pre-frail elderly women. Motricidade 12, 44–53.
Google Scholar
Ribeiro, A. S., Schoenfeld, B. J., Pina, F. L. C., Souza, M. F., Nascimento, M. A., dos Santos, L., et al. (2015). Resistance training in older women: Comparison of single vs. multiple sets on muscle strength and body composition. Isokinet. Exerc. Sci. 23, 53–60. doi:10.3233/IES-140564
CrossRef Full Text | Google Scholar
Rikli, R. E., and Jones, C. J. (2013). Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 53, 255–267. doi:10.1093/geront/gns071
PubMed Abstract | CrossRef Full Text | Google Scholar
Sardeli, A. V., Tomeleri, C. M., Cyrino, E. S., Fernhall, B., Cavaglieri, C. R., and Chacon-Mikahil, M. P. T. (2018). Effect of resistance training on inflammatory markers of older adults: A meta-analysis. Exp. Gerontol. 111, 188–196. doi:10.1016/j.exger.2018.07.021
PubMed Abstract | CrossRef Full Text | Google Scholar
Schott, N., Johnen, B., and Holfelder, B. (2019). Effects of free weights and machine training on muscular strength in high-functioning older adults. Exp. Gerontol. 122, 15–24. doi:10.1016/j.exger.2019.03.012
PubMed Abstract | CrossRef Full Text | Google Scholar
Schulz, K. F., Altman, D. G., and Moher, D.the CONSORT Group (2010). CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 8, 18. doi:10.1186/1741-7015-8-18
PubMed Abstract | CrossRef Full Text | Google Scholar
Signorile, J. F., Sandler, D., Ma, F., Bamel, S., Stanziano, D., Smith, W., et al. (2007). The gallon-jug shelf-transfer test: An instrument to evaluate deteriorating function in older adults. J. Aging Phys. activity 15 (1), 56–74. doi:10.1123/japa.15.1.56
CrossRef Full Text | Google Scholar
Straight, C. R., Lindheimer, J. B., Brady, A. O., Dishman, R. K., and Evans, E. M. (2016). Effects of resistance training on lower-extremity muscle power in middle-aged and older adults: A systematic review and meta-analysis of randomized controlled trials. Sports Med. 46, 353–364. doi:10.1007/s40279-015-0418-4
PubMed Abstract | CrossRef Full Text | Google Scholar
Tomeleri, C. M., Souza, M. F., Burini, R. C., Cavaglieri, C. R., Ribeiro, A. S., Antunes, M., et al. (2018). Resistance training reduces metabolic syndrome and inflammatory markers in older women: A randomized controlled trial. J. Diabetes 10, 328–337. doi:10.1111/1753-0407.12614
PubMed Abstract | CrossRef Full Text | Google Scholar
Vale, R. G. de S., Pernambuco, C. S., Novaes, J. S., and Dantas, E. H. M. (2006). Teste de Autonomia Funcional: Vestir e Tirar Uma Camiseta (VTC). Rev. Bras. Ciênc. E Mov. 14, 71–78. doi:10.18511/0103-1716/rbcm.v14n3p71-78
CrossRef Full Text | Google Scholar
Van Roie, E., Walker, S., Van Driessche, S., Delabastita, T., Vanwanseele, B., and Delecluse, C. (2020). An age-adapted plyometric exercise program improves dynamic strength, jump performance and functional capacity in older men either similarly or more than traditional resistance training. PLOS ONE 15, e0237921. doi:10.1371/journal.pone.0237921
PubMed Abstract | CrossRef Full Text | Google Scholar
Vasconcelos, A. B. S., Resende-Neto, A. G., Nogueira, A. C., Aragão-Santos, J. C., Monteiro, M. R. P., Morais Junior, G. S., et al. (2020). Functional and traditional training improve muscle power and reduce proinflammatory cytokines in older women: A randomized controlled trial. Exp. Gerontol. 135, 110920. doi:10.1016/j.exger.2020.110920
PubMed Abstract | CrossRef Full Text | Google Scholar
Vestergaard, S., Patel, K. V., Bandinelli, S., Ferrucci, L., and Guralnik, J. M. (2009). Characteristics of 400-meter walk test performance and subsequent mortality in older adults. Rejuvenation Res. 12, 177–184. doi:10.1089/rej.2009.0853
PubMed Abstract | CrossRef Full Text | Google Scholar
Vlietstra, L., Hendrickx, W., and Waters, D. L. (2018). Exercise interventions in healthy older adults with sarcopenia: A systematic review and meta-analysis. Australas. J. Ageing 37, 169–183. doi:10.1111/ajag.12521
PubMed Abstract | CrossRef Full Text | Google Scholar
Wolf, R., Locks, R. R., Lopes, P. B., Bento, P. C. B., Rodacki, A. L. F., Carraro, A. N., et al. (2020). Multicomponent exercise training improves gait ability of older women rather than strength training: A randomized controlled trial. J. Aging Res. 2020, 6345753–6345758. doi:10.1155/2020/6345753
PubMed Abstract | CrossRef Full Text | Google Scholar
link