

This systematic review was conducted by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines18. The primary aim was to systematically identify, appraise, and synthesize evidence from studies investigating the effects of CE protocols on functional outcomes, knee pain, and biomechanical parameters in individuals with ACLR. The review protocol was prospectively registered in the PROSPERO database (CRD42024608173).
Search strategy
We identified the relevant studies through 4 electronic databases: PubMed, Web of Science, Scopus, and Embase. The search was run on May 3, 2025. Key terms used in the search strategy were based on broad terms and related synonyms targeting 3 categories: #1 “anterior cruciate ligament” or ACL #2 “core stabili*” or “core strength*” or “hip strength*” or “hip focused” or “trunk focussed” or core #3 pain or gait or function* or activit* or biomechanic* #4 (1 AND 2 AND 3). We hand-searched reference lists from previous related systematic reviews on CE and function for ACLR to ensure identification of all relevant studies.
Eligibility criteria
Studies were included based on the following PICO criteria:
Population: participants with a history of ACLR, regardless of post-ACLR time, age, or surgery type.
Intervention: any form of strength exercises targeting knee functional performance, biomechanical outcomes, and knee pain.
Comparators: any control intervention (e.g., traditional exercise, rehabilitation, standard exercise, or physiotherapy standard).
Outcomes: primary outcomes included objective pain measures as VAS, KOOS-pain. Secondary outcomes included objective functional, biomechanical, and self-reported assessments using a validated questionnaire.
Study design: randomized controlled trials (RCTs).
Study selection
All records retrieved through the search strategy were imported into RevMan, and duplicates were subsequently removed. Titles and abstracts were independently screened by MJB and FK to select potentially relevant studies. Full-text articles of eligible studies were then obtained and assessed according to the predefined inclusion criteria. Any discrepancies between reviewers were resolved by consensus or, if needed, through consultation with a third reviewer (SHM).
Quality assessment
Methodological quality of the included studies was assessed by (MJB and FK) using the PEDro checklist, which consists of 11 items19. The PEDro Score had illustrated “fair” to “excellent” inter-rater reliability (ICC = 0.53 to 0.91) and “excellent” inter-rater reliability (ICC = 0.80 to 0.89) for clinical trials of physiotherapy-related interventions20. It has been suggested that scores of < 4 are considered “poor”, 4 to 5 are considered “fair”, 6 to 8 are considered “good”, and 9 to 10 are considered “excellent”20. Disagreements were resolved either through a third reviewer (SHM) or via consensus-based discussion when necessary.
Risk of bias
The methodological quality of the included studies was evaluated by two assessors (MJB and FK) using the RoB 2 risk of bias, which consists of 5 items19. The RoB 2 tool has been shown in five distinct domains. Within each domain, users of RoB 2 answer one or more signaling questions. These answers lead to judgments of “low risk of bias,” “some concerns,” or “high risk of bias”.
Data collection
MJB extracted all data from the included studies, and (SHM) verified all data. Function, pain, and lower-limb biomechanics data, including IKDC, Lysholm, Tegner, VAS, goniometer, hopping tests, and gait analysis, commonly used in the management of ACLR in the clinical setting, were extracted. Study design, number of sessions, intervention, variables, number of participants, and features, age, sex, height, mass, task, and tools were extracted from the included studies.
Synthesis of results
Mean differences and 95% confidence intervals (CI) were determined using a random effects model in RevMan version 5.4. A meta-analysis was carried out when two or more studies examined the same outcome measure with similar methodologies. The statistical heterogeneity of the combined data was assessed through I² statistics and corresponding P-values (P < 0.05). Results were interpreted based on the levels of evidence established by Tulder et al.21 modified by Mousavi et al.22 (Table 1).
Study selection
The literature search yielded a total of 736 items (PubMed (169 studies), Web of Science (138), Scopus (292), and Embase (137)) from which 229 studies remained after duplicate removal. After screening the titles and abstracts, 10 studies were included. Ten studies were assessed23,24,25,26,27,28,29,30,31,32. Figure 1 shows the flow diagram of the selection process and the number of excluded studies at each stage.
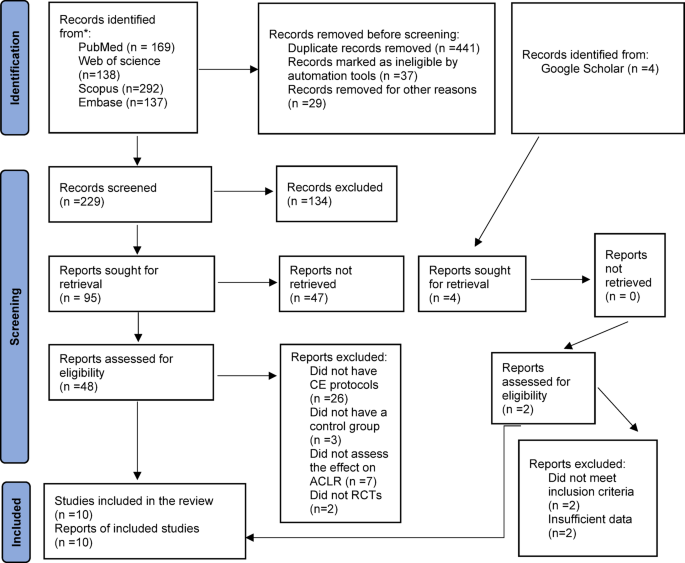
Flow chart of the study selection process.
Study characteristics
Table 2 summarizes the characteristics of the included studies. The designs of the included studies consisted of 10 RCTs (level-2 evidence)23,24,25,26,27,28,29,30,31,32. The total sample size of included studies was 463.
Quality assessment
Table 3 shows the results of quality assessment using the PEDro scale. The average score of eligible studies was 7.4. There were two studies of excellent quality27,30 which had concealed allocation and similar participants at baseline, 8 studies with good quality23,24,25,26,28,29,32,33. The majority of outcomes (n = 5) were graded as high; exceptions included the Tegner scale, pain outcomes, which demonstrated moderate-level ratings (supplementary file 1).
Risk of bias
Table 4 shows the results of risk of bias using the RoB 2 scale34. The overall risk of bias of eligible studies was high.
Outcome measured
Of the 10 studies, 10 targeted function23,24,25,26,27,28,29,30,31,32, 6 measured Pain24,27,28,29,30,31 and 2 studies targeted biomechanics23,32.
Effects of CE on performance
Ten studies investigated the effect of CE on performance, by a single-leg hop test25,27,28,30,32, triple hop test25,26,28,32, IKDC24,28,29, ROM29,30, Lysholm score23,31 and Tegner score26,31. The results of meta-analysis suggested strong evidence of significant increased changes in the combined single leg hop test score, triple hop test score (Fig. 2), and IKDC in the CE group compared to the traditional exercise group (Fig. 3). Furthermore, the meta-analysis results showed moderate evidence of significant changes in knee extension ROM (Fig. 4). Moderate evidence of a significant increase in overall IKDC, Lysholm score, and Tegner score26,31 in the CE group compared to the traditional exercise group. Limited evidence showed non-significant changes for one leg rise, side hop test, KOOS symptoms, KOOS-sport, KOOS-Qol, ACL-Qol, ACL-RSI, and KOOS4.

Results of the meta-analysis of the hop test score between the CE group and the traditional exercise group.

Results of the meta-analysis of the Performance questionnaire between the CE group and the traditional exercise group.

Result of the meta-analysis of knee extension ROM between the CE group and the traditional exercise group.
Effects of CE on pain
Six studies investigated the effect of CE on pain; 4 studies measured pain by VAS28,29,30,31one measured pain by KOOS-pain27and one study measured pain by the HSS24. The results of the meta-analysis suggested strong evidence of non-significant changes in pain score for the CE group compared to the traditional exercise group (Fig. 5).

Result of the meta-analysis of the pain between the CE group and the traditional exercise group.
Effects of CE on lower-limb biomechanics
Two studies investigated the effect of CE on lower-limb biomechanics during gait23,32. Limited evidence showed a significant increase in swing-phase time on the affected side, peak reaction force of the hip, knee, and ankle23. Moreover, limited evidence showed a significant decrease in gait cycle time, stance-phase time on the normal side23. Furthermore, limited evidence showed non-significant changes for VGFR, A-PGFR, and M-LGFR32, in the CE group compared to the traditional exercise group.
link