

Participants
A group of 24 adults (5 women and 19 men; age, 36.7 ± 11.1 years, range 18–56 years; body mass, 86.7 ± 20.9 kg; height, 175.2 ± 10.2 cm) after ACL reconstruction met the inclusion criteria and were included in the study. Inclusion criteria: adult men and women who had sustained an acute knee injury resulting in a complete anterior cruciate ligament (ACL) rupture, confirmed by magnetic resonance imaging (MRI) and clinical examination. Eligible participants underwent ACL reconstruction within a period ranging from the day of injury up to 12 months post-injury. All participants were medically cleared to begin a structured postoperative rehabilitation program. Exclusion criteria – participants were excluded if they presented with any of the following conditions: history of previous knee surgery or ACL reconstruction on the same (injured) limb, concomitant injury to other major knee structures (e.g., posterior cruciate ligament, collateral ligaments, menisci requiring repair, articular cartilage damage), chronic or degenerative joint diseases (e.g., osteoarthritis, rheumatoid arthritis), neuromuscular or musculoskeletal disorders affecting lower limb function, systemic diseases influencing muscle or connective tissue function, any contraindications to physical exercise or participation in resistance training, or lack of adherence to the full rehabilitation protocol. In addition, patients requiring multistructural or multitissue surgical procedures were excluded. Multiligamentous knee injuries, articular cartilage damage, or unstable meniscal tears constituted exclusion criteria. The presence of a concomitant stable medial meniscal tear was not considered an exclusion criterion, provided that it did not require surgical repair or modification of postoperative recommendations and the standardized rehabilitation protocol.
The participants were randomly allocated into two groups: a standard rehabilitation group (SR; n = 12) and a standard rehabilitation plus inertial exercises group (SRI; n = 12). (Table 1). Participants were randomly allocated to the SR or SRI group using simple randomization (lottery method). After eligibility was confirmed (24 of 38 screened participants), group assignment was performed by an independent person not involved in recruitment, intervention delivery, or outcome assessment. Randomization was conducted prior to baseline assessments. Due to the nature of the intervention, participants and physiotherapists were not blinded; however, outcome assessments were conducted by two independent assessors blinded to group allocation. Each participant was qualified for ACL reconstruction surgery as a result of different acute injuries (football: n = 12, skiing: n = 4, basketball: n = 1, volleyball: n = 1, kickboxing: n = 2, traffic accident: n = 3, and playing with children: n = 1). Participant recruitment, group allocation, follow-up, and analysis are summarized in a flow diagram, (Fig. 1). All surgeries were performed by the same physician using the same procedure (described below). Each subject participated in 12-week rehabilitation in the same rehabilitation company. Rehabilitation was carried out by the same two physiotherapists twice a week for approximately 60 min per session. Subjects from the SR group performed standard rehabilitation applied by the rehabilitation company (described below), while SRI performed the same rehabilitation and additionally performed inertial exercises from the seventh week of rehabilitation. This study was designed as a pilot randomized controlled trial. Given its exploratory nature, no formal a priori sample size calculations were performed. The sample size was determined pragmatically based on the number of eligible patients who met the inclusion criteria and were recruited during the predefined study period. This study was approved by the Bioethics Committee of the Collegium Medicum University of Zielona Góra (approval no. RCM-CM-KBUZ031.13.2022), Poland. All procedures were performed in accordance with the Declaration of Helsinki and relevant national regulations. Written informed consent was obtained from all participants prior to participation. The trial was prospectively registered at ClinicalTrials.gov (identifier: NCT06726044; date of registration: 12.05.2024).
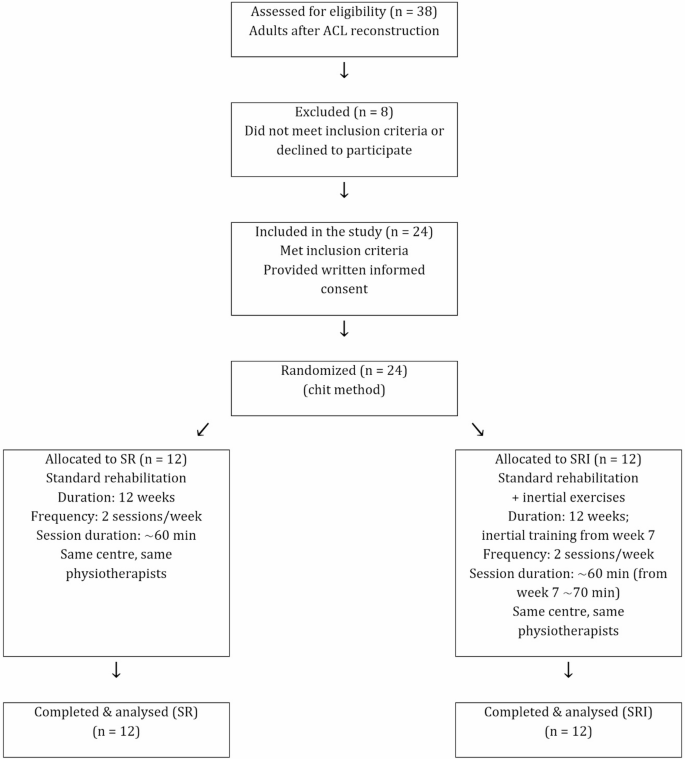
Flow diagram of participants.
Surgical technique
All anterior cruciate ligament reconstructions were performed arthroscopically with the patient in the supine position under tourniquet control. An autograft harvested from the semitendinosus and gracilis tendons was used in each case. After harvesting, the grafts were appropriately prepared and configured for implantation into femoral and tibial bone tunnels. No synthetic tape or suture-augmentation devices were used. Following standard arthroscopic inspection of the knee joint, femoral and tibial tunnels were created using dedicated instruments. Femoral fixation was achieved using a cortical suspension device (Ultrabutton, Smith & Nephew), and tibial fixation was performed using a titanium interference screw (SoftSilk, Smith & Nephew). In cases where a concomitant stable medial meniscal tear was identified, meniscal repair was performed using an all-inside technique with the Fast-Fix 360 system (Smith & Nephew). All patients received a compressive dressing and a surgical drain, which was removed on the first postoperative day. The skin sutures were removed 14 days after the surgery.
Rehabilitation
All participants completed a 12-week standard rehabilitation program including manual therapy (mobilization of the patella and fibular head, myofascial release, manual scar treatment, osteopathic techniques), anti-swelling interventions (manual lymphatic drainage, compression, cryotherapy), kinesiotaping, joint activation exercises, flossing, and kinesiotherapy. Exercises included strength training and knee flexion–extension performed in both closed and open kinetic chains, as well as isometric quadriceps exercises through the full range of motion.
From the seventh to the twelfth week of rehabilitation subjects from SRI additionally to standard rehabilitation program performed inertial exercises. Due to safety considerations during the early postoperative phase, inertial exercises were deliberately implemented in a closed kinetic chain configuration to ensure controlled load transmission across the knee joint. For this purpose, a dedicated inertial rehabilitation device (InerKnee – Fig. 2) was designed and manufactured within the framework of the present research project to enable inertial knee extension training under closed kinetic chain conditions in a seated position. More details concerning this device are provided in Strength measurements section. Inertial exercises were performed twice a week, 4 sets of exercises, each lasting 15 s, 2 min rest periods between sets were used. Range of motion was 60 degrees. Before including inertial exercises to rehabilitation maximal strength of knee extensors of uninvolved limb under inertial conditions was evaluated. During the first two weeks of inertial exercises performed by involved limb a load of 60% of the maximal strength obtained by the uninvolved limb was used. Then, every two weeks of inertial exercises the load was increased by 10% so during the last two weeks it was 80% of the maximum force of the uninvolved limb. All inertial exercises were performed under the same physiotherapist supervision to ensure proper technique and safety.

InerKnee – inertial rehabilitation device.
Measurements
Baseline assessments were performed two weeks post-surgery and included body height, body mass, thigh circumference, and body composition. Pre-intervention strength testing of the operated limb was not performed due to safety considerations in the early postoperative phase, when maximal voluntary efforts could potentially compromise graft protection and patient comfort. After rehabilitation, these measures were repeated, and additional assessments of isokinetic knee extensor and flexor strengths, inertial knee extensor strength, and dynamic balance were performed.
Thigh circumference
Measurement of thigh circumference was accomplished with the patient in the supine position with the knee fully extended. Both the uninvolved and the involved limb were assessed. The circumference of the thigh was measured with a tape measure at points of 5.0 cm, 10.0 cm, and 15.0 cm, proximal to the superior pole of the patella, by the same examiner with each made to the nearest 0.5 cm. According to the protocol used by Yoshii et al.26, the thigh circumference was assessed at 5, 10, and 15 cm above the patellar border. However, during measurements, 5 cm above the patella, a swelling effect was observed, resulting in disproportionately high early postoperative circumferences that did not represent true muscular changes following rehabilitation. Therefore, only the 10- and 15-cm measurements were considered and included in the primary statistical analysis. The same researcher took three measurements, with each made to the nearest 0.5 cm. The mean value of the three measurements was used for future calculations.
Body composition
To evaluate the influence of rehabilitation on body composition, a bioelectrical impedance device (Tanita MC-980 MA; Tanita Corporation, Tokyo, Japan) was used. The subjects were asked to maintain a normal state of hydration prior to the measurements, and they were not allowed to exercise or eat for 12 h preceding the measurements. The measurements were made in the morning according to the manufacturer’s guidelines.
Strength measurements
Maximal voluntary torque (MVT) under isokinetic conditions.
The maximal torque derived from isokinetic muscle actions was determined using a specialized Biodex 4 Pro device (Shirley, NY, USA). Data collection was preceded by a familiarization session. Measurements were collected in a seated position. During measurements, the ankle of the active leg was attached to the Biodex 4 Pro device moving shin pad. In the starting position, the thigh of the active leg was immobilized at 90 degrees in relation to the trunk, and the knee was positioned at 60 degrees (180 degrees corresponded to complete maximal extension of the knee joint). To prevent any activity of other muscle groups that were not being tested, the participant’s trunk was stabilized using belts across the chest. Measurements were performed at two velocities 60°/s and 180°/s with a 2-min rest period between measurements. During both measurements, first the healthy leg and then the operated leg were tested. Each measurement began with two trial cycles, each composed of extension and flexion of the knee joint, followed by five repetitions involving maximal strength. Prior to the measurements, the participants were given verbal instructions regarding the experiment’s design. The highest value among the five maximal trials of each measurement was adopted for further analysis.
The maximal force under inertial conditions.
The measurements were made using InerKnee device (Fig. 2). This device was designed and manufactured as part of a publicly funded research and development project focused on the development of an innovative, inertial rehabilitation protocol following arthroscopic ACL reconstruction. The device concept was informed by prior inertial systems. Unlike common flywheel systems typically used in open kinetic chain configurations, InerKnee enables inertial loading under closed kinetic chain conditions. The device demonstrates high test–retest reliability (intraclass correlation coefficient consistency ≥ 0.941, ICC agreement ≥ 0.923). Measurements were preceded by two familiarization sessions to ensure proper technique and minimize potential task-specific learning effects. After warm-up, each participant performed a 10-second maximal test of the knee extensors. First test was performed at the start of inertial rehabilitation (7th week of rehabilitation) and only healthy leg was tested. At the end of rehabilitation first the healthy leg and then the operated leg were tested with a 1-minute break between measurements. All tests were performed while seated in a rehabilitation chair. The range of motion for each exercise was approximately 60 degrees. All measured parameters (force, range of motion, etc.) were recorded using a computer and displayed in real time on the screen. The maximal value of force (in newtons) achieved during one full cycle was used for further analysis.
Star Excursion Balance Test (SEBT)
Dynamic balance was assessed using the SEBT according to the methodology described by Bulow et al.27. Participants completed a warm-up consisting of five minutes of brisk walking on a treadmill, followed by a dynamic stretching routine. The patients performed three practice trials and three measurement trials of the SEBT for both legs. The average of the three measurements was used for the data analysis (in cm). The patients stood barefoot with both hands placed on their hips. The patients were instructed to reach their foot and touch the tape as far as possible in the anterior (ANT), posteromedial (PM), and posterolateral (PL). A standardized order of testing was utilized, the uninvolved limb was measured first in the order of ANT, PM and PL. Testing was repeated in the same order for the involved stance limb. The tester provided patient feedback and proper guidance to reduce mistakes during practice trials. The SEBT – ANT, PM, PL, and composite scores were used for the analyses. The SEBT scores were normalized to the limb length measurement of the patients.
All interventions were well tolerated, and no adverse events were observed during the rehabilitation period.
Statistical analysis
The Shapiro–Wilk test was used to assess the normality of data distribution. Descriptive statistics are presented as means ± standard deviations. For variables assessed both before and after the intervention (thigh circumference and body composition parameters), a two-way repeated-measures analysis of variance (RM-ANOVA) was performed, with time (pre vs. post) as the within-subject factor and group (SR vs. SRI) as the between-subject factor. When significant main effects or interactions were detected, the Scheffé post hoc test was used to identify pairwise differences. To further characterize the magnitude of training effects, relative changes (%) were calculated for each participant. Between-group differences in relative changes were analyzed using independent-samples t-tests. For outcomes assessed only after rehabilitation (isokinetic strength, inertial strength, and dynamic balance), between-group comparisons were conducted using independent-samples t-tests.
Effect sizes (ES) were calculated using Cohen’s d. Within-group effect sizes were computed for pre–post comparisons using dependent-samples Cohen’s d, whereas between-group effect sizes were calculated based on relative change (%) scores. Effect sizes were interpreted according to Cohen’s criteria: d < 0.41 (small), 0.41–0.70 (moderate), and > 0.70 (large)28. The level of statistical significance was set at p ≤ 0.05.
link